75 year old with fever under evaluation
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Case seen by Unit 5 :
M. Sridevi (Intern)
Anjali Vishwas( Intern)
Mourya ( Intern)
Shriya ( Intern)
Dr. Praveen Naik Sir( Ass professor)
Dr. Natasha Mam
Dr. Zain Alam Sir
Dr. Sashikala mam
Dr. Shailesh Patil Sir
Here is the case I have seen :
Complaints and duration:
A 76 year old female presented to opd with complaints of fever since 1 year, complaints of vomiting s since 1 month, tingling sensation of bilateral upper and lower limb since 1 week, loss of appetite since 1 year
Patient was apparently asymptomatic 1 year ago, then she developed fever which is sudden in onset, gradually progressive ik nature, associated with chills and rigors, subsided on taking medication.
History of fever every month since 1 year which subsides on taking medication
Complaints of vomitings since 1 month ( 10 to 12 episodes in a day, bilious in type, containing food particles, is non projectile subsides on taking medication.
Complaints of tingling sensation of bilateal upper and lower limbs since 1 week
Complaints of loss of appetite since 1 year
History of burning micturition 1 month back
History of cough 15 days ago, associated with sputum, scanty in amount, no diurnal variation seen relieved with medication
History of lower abdominal pain diffuse , squeezing type, radiating to back 1 month ago relieved on Taking medication
No complaints of chest pain, palpitations, giddines, cold, cough, burning micturition, pedal edema, headache , loose stools, no dysuria
Past medical and surgical history:
K/c/0 diabetes since 14 years and is on T. Glycomet -GP2
Not a known case of HTN, Epilepsy, TB, thyroid abnormalities, any other systemic illness
No history of previous blood transfusion
History of cataract surgery in both eyes
Personal history: Appetite decreased since 1 year
Bowel movement s regular, micturition normal, no known history of allergies,
No addictions
Family history: not significant
Vitals at the time of admission:
Bp: 110/80 mm hg, PR:76 bpm, RR: 22 cpm
Investigation s:
Hemogram




Rbs: in normal range



 Cbnaat report
Cbnaat report

 FBS
FBS
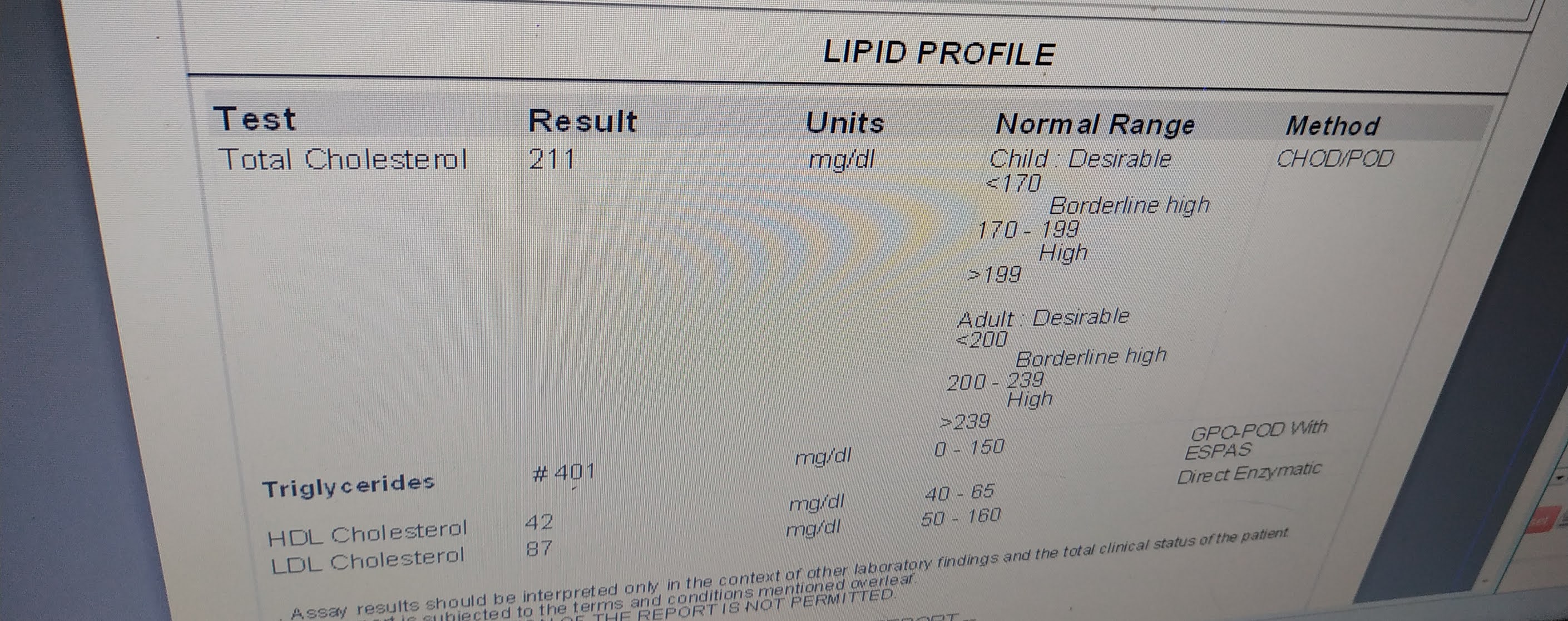
 Fasting lipid profile : showing elevated triglycerides
Fasting lipid profile : showing elevated triglycerides
 PlBS
PlBS
 Serum potassium: hypokalemia noted
Serum potassium: hypokalemia noted

Ophthalmology referral in view of Diabetic retinopathy changes

Usg abdomen and pelvis

Chest X ray

Rntcp report


HIV testing

Awaiting for blood culture and sensitivity reports
Diagnosis: FEVER UNDER EVALUATION ASSOCIATED WITH COUGH WITH SPUTUM
Treatment given:
Tablet PCM 500 mg PO/SOS
Temperature monitoring
Inj. HAI S/C (8 AM , ---2PM---8 PM)
Grbs monitoring( before breakfast, 2 hrs after breakfast, before lunch, 2 hrs after lunch, before dinner, 2 hrs after dinner, at 2 am in the morning)
Tablet Doxycycline 500 mg /BD/PO
Day. 2 INVESTIGATION S
ESR: elevated






Awaiting for blood culture and sensitivity reports
Thanks for sharing this very nice blog with us. This is super informative. I just love it. This post is going to be very helpful for so many people. Check out the site for best doctor for fever treatment.
ReplyDelete